








.webp?width=387&height=387&name=Medtech%20Breakthrough%20Award%20Winner%20(1).webp)




























Provider Roster Reconciliation That Catches Payer Errors Before Claims Do

Summarize This Article With
A health plan can pass a network adequacy filing and still fail its members. The directory looks complete on paper, yet listed phone numbers ring to the wrong offices and a share of the named clinicians stopped accepting new patients months ago. Most payer operations teams already know this gap exists. What they tend to underestimate is how much manual effort goes into keeping even a flawed directory from getting worse, and how little lasting accuracy that effort actually buys.
Provider directory automation changes the math. Instead of treating accuracy as a quarterly cleanup project, it builds verification into the daily flow of provider data.
This guide walks through what automation replaces, where manual programs break down, and how to evaluate a model that holds up under CMS scrutiny.
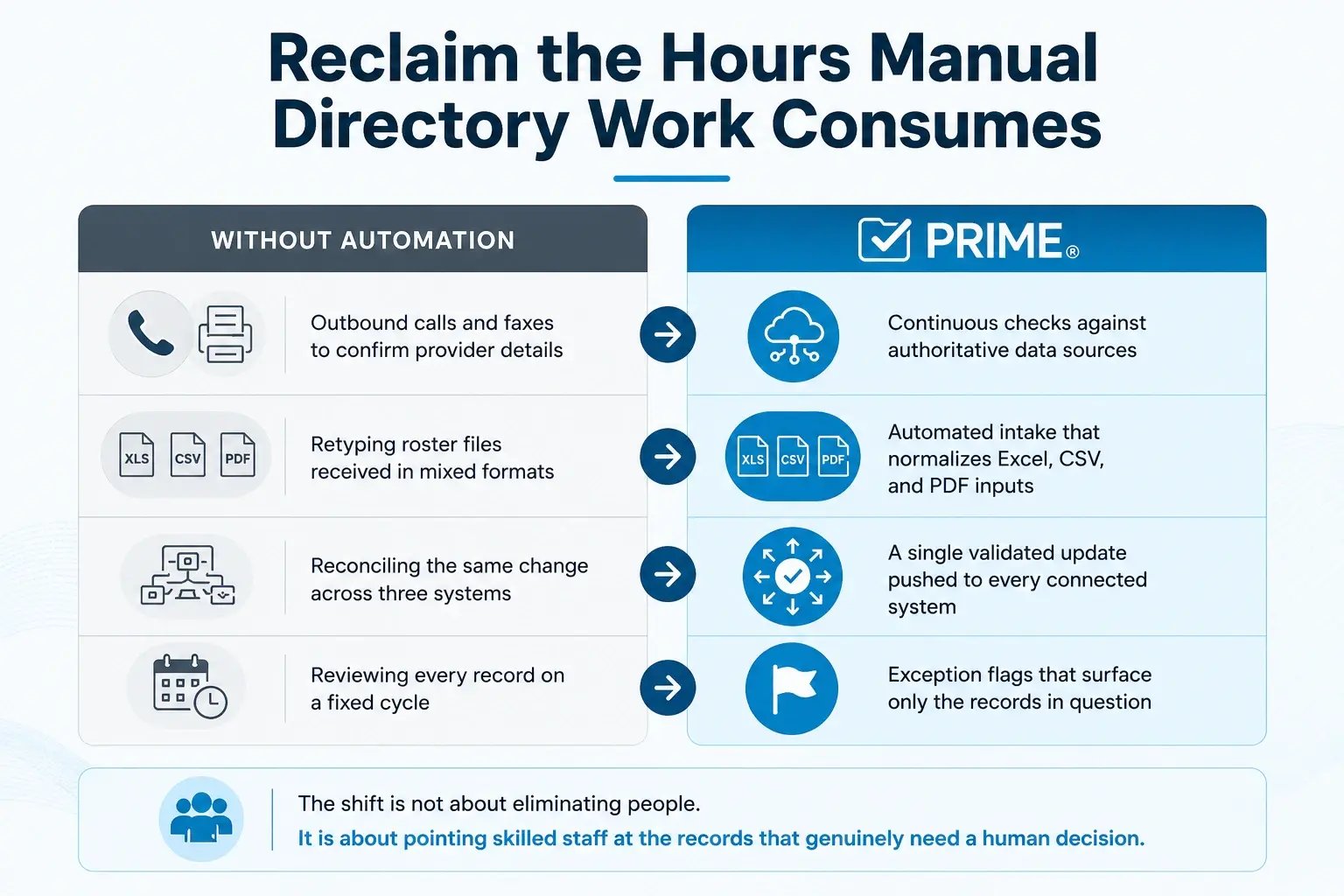
Reclaim the Hours Manual Directory Work Consumes
Most directory teams spend their week on work that produces no durable accuracy. They chase providers by phone and fax, retype roster files that arrive as PDFs or scanned spreadsheets, and reconcile the same address change across credentialing, claims, and the public directory, one record at a time. The effort is real, but it scales linearly with network size, which means a growing plan simply hires more people to stay in the same place.
Automation removes the repetitive layer of that work and lets your team focus on judgment calls instead.
See how it works. Get a 30-minute PRIME® demo
Spot Where Manual Maintenance Quietly Breaks Down
Manual directory programs rarely fail loudly. They erode, because the process depends on conditions that almost never hold across a large network.
Providers don’t have a direct incentive to prioritize a verification request among competing administrative demands, so response rates stay low. When a clinician participates in several networks, the same update has to be submitted to each plan separately, and information confirmed to one plan does not propagate to the others. Roster files arrive in inconsistent formats, which forces manual cleanup before the data is even usable. On top of that, batch verification cycles introduce lag, so a directory can be technically current at the start of a quarter and materially wrong by the end of it.
That lag is the real problem. Federal rules expect updates to reach the public directory within two business days of receiving new information, and a phone-and-spreadsheet process simply cannot move at that speed across thousands of records.
Get Ahead of the Mandates Reshaping Directory Compliance
Regulatory pressure is no longer the reason to consider automation. It is the reason to move now. Three forces are converging, and they are escalating in step.
The REAL Health Providers Act sets the clearest signal. It directs CMS to require Medicare Advantage organizations to maintain accurate, regularly verified provider directories, with removal of unverified listings and stronger oversight of accuracy. It is the first federal law written specifically to hold MA plans accountable for directory quality, which makes it the mandate most directly aimed at the workflows automation is built to fix.
Alongside it, CMS finalized rule CMS-4208-F2 requires Medicare Advantage organizations to submit provider directory data directly to CMS for publication on Medicare Plan Finder, which raises the stakes on data quality and timeliness.
CMS also expects plans to verify directory information at regular intervals, with a 90-day standard widely applied across programs, while Section 116 of the No Surprises Act, enacted through the Consolidated Appropriations Act, 2021, shifts financial risk to plans when members rely on inaccurate listings.
The financial exposure runs deeper than penalties. Stale provider data lowers first-pass claims rates, drives grievances, and invites corrective action plans that consume leadership attention for months.
Choose Capabilities That Actually Move Accuracy
Vendor demos tend to blur together, so it helps to evaluate against the capabilities that change accuracy outcomes rather than the ones that simply look modern.
- Automated collection from multiple authoritative sources, including provider websites, so verification does not depend on outreach response rates
- A defined source-of-truth hierarchy that decides which input wins when two sources disagree
- Exception-based review that routes only uncertain records to staff and clears the rest automatically
- Bidirectional sync through FHIR-compliant APIs so credentialing, claims, and the public directory stay aligned
- A provider self-service portal that lets clinicians confirm their own details and reduces inbound data entry
- A time-stamped audit trail of every change and verification, ready for regulator review
A platform missing the source-of-truth logic or the audit trail will move data quickly without making it more trustworthy, which defeats the purpose.
Trace How Automation Keeps Every Listing Current
It helps to follow a single update through an automated pipeline, from raw input to the listing a member sees.
The process starts when data enters the system, whether from a provider portal, a delegated roster, or an automated source check. The platform normalizes that input into a consistent format regardless of how it arrived. It then validates each field against authoritative sources and assigns a confidence score to the result. High-confidence updates flow straight through, while low-confidence records are flagged for staff review. Once a record is approved, the platform pushes it to every connected system in one motion, so the directory, the claims platform, and the credentialing record never drift apart.
This is what closes the timeliness gap. Verification runs continuously in the background instead of waiting for a scheduled cycle, which is the only realistic way to meet a two-business-day update expectation at network scale.
Build a Business Case Finance Will Approve
A directory automation proposal lands better when it speaks the language of return rather than the language of tooling. Three value streams carry most of the case.
The first is labor reallocation. Staff hired for analysis and provider relations spend much of their week on data entry, and automation returns those hours to higher-value work without expanding headcount.
The second is claims performance, because cleaner provider demographics raise first-pass rates and reduce the rework that follows mismatched submissions.
The third is avoided exposure, since accurate directories lower the risk of penalties, corrective action plans, and the Star rating damage that follows member complaints.
Add the reduction in outbound outreach cost once providers maintain their own records, and the model usually pays back well inside the window most finance teams require for an operations investment.
Decide Whether to Build, Buy, or Blend
The delivery model matters as much as the capability set. Each path carries a real tradeoff.
|
Approach |
Best fit |
Main tradeoff |
|
Build in-house |
Plans with strong HL7 and FHIR engineering and a long runway |
A 12 to 18 month path to production, plus ongoing maintenance you own |
|
Buy a platform |
Plans facing near-term CMS deadlines and limited internal capacity |
Less control over the underlying data model and feature roadmap |
|
Hybrid |
Plans with capable teams but compressed timelines |
Requires clear ownership lines between internal and vendor scope |
For most plans working against the 2027 Medicare Plan Finder timeline, building from scratch is difficult to justify, because the runway alone can exceed the deadline. The practical question is usually how much of the workflow to keep in-house around a purchased core..
Sustain Accuracy With a Modern Operating Model
A mature directory operating model looks different from the one most plans run today. Verification is continuous rather than periodic. Staff work from an exception queue instead of reviewing every record on a calendar. Accuracy is a tracked metric with an owner, not an assumption that resurfaces only during an audit. Provider, credentialing, roster, and affiliation data live in one system, so a single confirmed change reaches every downstream destination.
This is the gap an automation platform is meant to close. Continuous monitoring is the feature that holds the model together, since it catches a provider who has retired, moved, or stopped accepting patients before a member ever encounters the error.
PRIME® by Atlas Systems is built around that continuous model, unifying provider data management and validation so directories stay current between audits rather than only during them.
The shift from manual maintenance to automation is no longer optional for plans serious about compliance and member trust.
Start your Provider Directory Automation Journey with PRIME®.

Related Reading
Blogs

















.webp)













.png)

